
New Fast Tests and Distress from Regulators
Abbott have received emergency FDA authorisation for a new fast test. What does it all mean?

Welcome to Plugging the Gap (my email newsletter about Covid-19 and its economics). In case you don’t know me, I’m an economist and professor at the University of Toronto. I have written lots of books including, most recently, on Covid-19. You can follow me on twitter (@joshgans) or subscribe to this email newsletter here.
Today’s news is all about testing and so we are back on that topic. To recap, if we want to deal with Covid-19 quickly and reduce economic pain, the only near-term solution is widespread frequent testing. The challenges are: (1) that we need cheap, rapid tests and (2) that we need regulators to change their incorrect approach to scoring such tests for the purposes of informing on pandemic mitigation (as opposed to Covid-19 treatment). Abbott has received FDA emergency authorisation for a $5 fast test that can be performed without special equipment; making it progress on (1). But it isn’t progress on (2) because their test is only authorised for use of symptomatic individuals. Given that our challenge is how to identify infected people we don’t otherwise expect to be infected, this limitation restricts the test’s usefulness for pandemic mitigation. So today’s post is about regulatory frustration.
The Abbott Test
First, the Abbott test itself. The BinaxNow™ COVID-19 Ag Card is a card where you can deposit the materials for a nasal swab (and not that deep stuff but what the experts will tell you is ‘picking distance’). It comes with an app where you can have the results recorded to use later to show you are positive or negative as the case may be.

Abbott claims they will be able to produce 50 million of these by October. That’s a lot. To put it in context, as of today, the US has performed almost 80 million tests in total.
The bottleneck in all of this won’t be the tests themselves but the fact that they can only be administered by healthcare providers. When you do that, you can then have the results recorded on an app. But your 15-minute test turns into something much longer when you need a separate trip to get one. In other words, at the moment, this is a cheap and rapid result solution — which is great — but it requires a limited set of skilled people to administer which reduces its potential. (It is an open question as to whether non-professionals could administer the test. I don’t know so I won’t weigh in on that … yet). Anyhow here is what the test results will look like.

They look … familiar … to anyone who has seen a pregnancy test.
I should note at this point that Health Canada has recently come out with a statement claiming that such tests would be unlikely to be authorised for home use.
The federal health agency worries that, “without the guidance of a health-care professional,” people would use the home test kit improperly or “misinterpret the results” and that it could be impossible to collect test results — information that’s key to “important health decisions involving disease control during an outbreak,” the department said in an emailed statement.
“If it’s done in a haphazard way … you might actually create more problems, confusion than the actual benefits because you might get maybe a higher risk of false negative results,” Dr. Howard Njoo, Canada’s deputy chief public health officer, said Tuesday during a COVID-19 briefing.
This may be the case. I worry about home tests, not because they might be conducted poorly, but because of results reporting. However, what is the evidence that tests cannot be conducted or interpreted by people at home? Why is that the default hypothesis here? Surely, this is something we might have a study or two on but I don’t believe one exists. In other words, this is a belief and surely that isn’t a sufficient scientific approach to this question.
The FDA Authorisation
The FDA has authorised use of the test using an emergency accelerated process. But, and it is a big but, it is only authorised for use on symptomatic patients. The problem there is obvious — if we want to test to isolate people who are asymptomatic spreaders this restriction clearly flies in the face of that goal. That is not to say it is without use. With the flu season approaching, it will be useful to distinguish Covid-19 symptoms from flu symptoms although that could be achieved with a test for the flu as well. Also, symptomatic patients aren’t always isolated as strongly as they should be and so having fast results can help there.
The key question is: why is this test only authorised for symptomatic use? There are two candidate explanations (and both may be true). First, to get approval Abbott submitted results from a study of 102 patients (actually I am not 100% sure it was this as they report 102 nasal swabs) who were suspected of having Covid-19 received the Abbott test and the ‘gold-standard’ PCR test.

It is not a large sample but in only one case did BinaxNow produce a false negative which is why the sensitivity of the test (the probability that you will test positive if you are actually positive) was reported as 97.1%. This is a high number but we have to remember what it is based on.
Sensitivity is calculated by taking the number of people who TEST positive and divide it by the number of people who ARE positive. You can improve sensitivity in two ways. You can have a more sensitive test which increases the numerator or you can select candidates for testing who are unlikely to be negative (and so decrease the denominator). This is subtle but this second path can really impact on things when there are small numbers. For instance, suppose that in your sample, 50:50 were actually positive and negative. If your test is less likely to pick up a positive case than the benchmark test, then it is likely that you will have more false negatives in this case — say 2 rather than 1. In this case, your sensitivity score would have been 48/50 or 96%. If it was 3, it would have been 94%. The point here is that, if your test is likely to have more trouble picking up positive cases, it really helps to be testing on people likely to be positive in the first place.
The FDA understood this sampling issue and so its authorisation is only for use on a similar pool of patients that were tested — that is, symptomatic patients. What we don’t know is what Abbott knows about testing on broader samples.
But even if Abbott had provided a broader study, there is another reason why the test is only authorised for use on symptomatic patients: the CDC just changed its guidelines and now only recommends testing on symptomatic patients. So this precludes testing on the general population, asymptomatic or pre-symptomatic patients (which you want to do if you want to stop them from infecting others) and from people who are known to have been exposed to the virus (e.g., through contact tracing).
“I think it’s bizarre,” said Daniel Larremore, a mathematician and infectious diseases modeler at the University of Colorado Boulder. “Any move right now to reduce levels of testing by changing guidelines is a step in the wrong direction.”
Prior iterations of the C.D.C.’s testing guidelines struck a markedly different tone, explicitly stating that “testing is recommended for all close contacts” of people infected with the coronavirus, regardless of symptoms. The agency also specifically emphasized “the potential for asymptomatic and pre-symptomatic transmission” as an important factor in the spread of the virus.
The newest version, which was posted on Monday, amended the agency’s guidance to say that people who have been in close contact with an infected individual — typically defined as being within six feet of a person with the coronavirus and for at least 15 minutes — “do not necessarily need a test” if they do not have symptoms. Exceptions, the agency noted, might be made for “vulnerable” individuals, or if health care providers or state or local public health officials recommend testing.
Suffice it to say, if the guidance is to test with symptoms, it seems to be that such guidance would then be applied to fast tests such as Abbott’s. This may be a reason Abbott didn’t try for a broader authorisation.
Now, there may be some rationale to back this up that wasn’t reported in the media. One possibility is that it is part of the “most tests are garbage” statement by Bill Gates in that PCR test results are too slow and also more likely to pick up the end of a virus than the beginning anyway that makes them not worthwhile for anything other than treatment. In this case, if the tests are useless for mitigation, it does not make sense to suggest they be used for that. However, this is in the opposite direction that many have recommended which is to get better and faster tests. What signals is the CDC sending here for test developers?
A ray of hope
Regulations can be changed so we should not take this as the end of the story. So let’s return to what we might now know from the Abbott test. The study reports another interesting table.
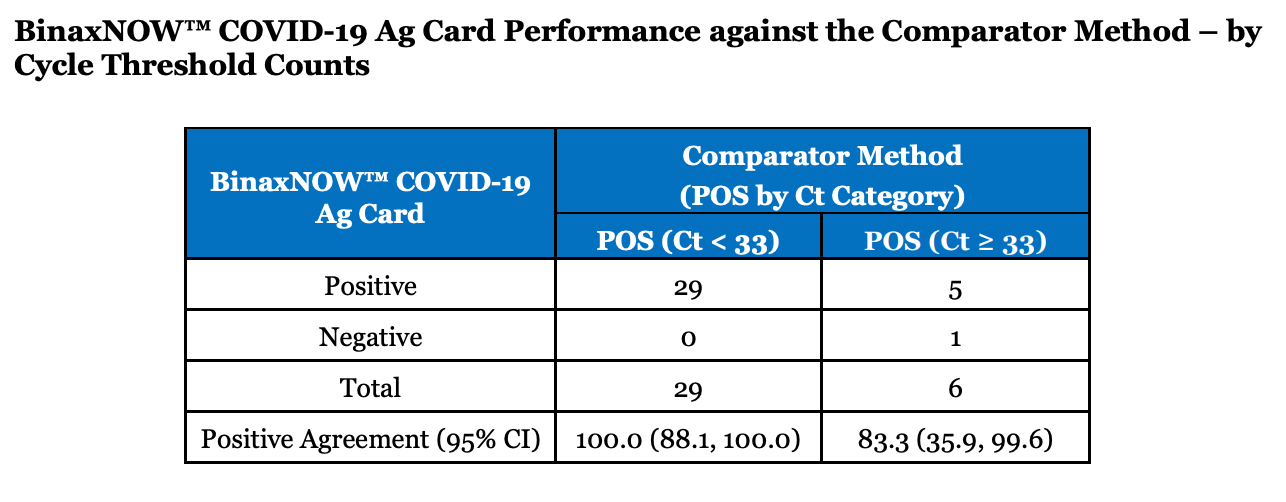
The Ct number is information regarding viral load with a lower number (meaning it took fewer PCR cycles to find the virus) meaning that viral load is higher. The table suggests that when there was a false negative, it was because the viral load in the patient was lower. In other words, the BinaxNow test picked up the patients with a higher viral load and hence, the ones most likely to be infectious. What this means is that BinaxNow may be a more valuable test for infectiousness than even a PCR test that would have more false positives on this dimension. (See my earlier post here).
Thus, we can add the Abbott test to the list of potential candidate tests that might be able to be widely deployed and used to identify infectious people quickly and isolate them and bring an end to this pandemic. How soon we can get to that point, however, appears to be in the hands of regulators.
Before you go, in case you are interested, I have a new paper that proves formally why tests for infectiousness like the Abbott test are more valuable for isolation decisions than PCR tests even if they are used once and didn’t have a speed advantage.