
Testing at the door versus testing at the desk

Welcome to Plugging the Gap (my email newsletter about Covid-19 and its economics). In case you don’t know me, I’m an economist and professor at the University of Toronto. I have written lots of books including, most recently, on Covid-19. You can follow me on twitter (@joshgans) or subscribe to this email newsletter here.
Given my focus on testing, I am sometimes asked how I might consider some operational details. If the goal is to have frequent (every 3 to 7 days) testing for various places like schools and offices, despite significantly positive rate of returns for these activities, there are some challenges. The usual presumption is that people will be tested before they enter a place — usually at the door. But with winter approaching, even with rapid tests, where do you put the people as they try and come in and wait for results? The winter issue makes it challenging to leave them outside. But waiting rooms are likely to become congested which is precisely what we don’t want.
An alternative would be to let people in and then test them at their desks (or wherever they happen to be). The advantages are obvious. No waiting at the door. You can spread testing personnel over the course of the day. And there are fewer operational challenges. This could make it an order of magnitude less costly to run. The disadvantage is also obvious. You are going to let infectious people into your place where they might spread the virus to others.
There are complications, however, to these simple costs and benefits. For instance, yes, you might let infectious people in but, if you are testing often, they are not in for long. The worse case is that they are there a day to do their worst. On the benefits side, if it is less costly to test at the desk, you can also test more often. Once you take into account this stuff, the choice between the two is less obvious.
Here is how I answered that question. In an earlier post, I described research by Ted Bergstrom, Carl Bergstrom and Haoran Li who did the maths on how the frequency of testing and delay in results impacted on the likely path of the virus. A rapid test done at the door involves no delay in results. What about a test at the desk? Technically, it also involves no delay in results but, instead, a delay in when someone is tested. If you let someone who is infected walk around for a day before getting a rapid test that is, in fact, the same as testing them and then letting them walk around for a day while they wait for the result. Thus, I could use that same maths to examine the potential cost of testing at the desk.
In doing so, I used this neat calculator they had set up. I assume that people still are careful with mask-wearing and social distancing inside so that R = 1.25 (which is the high end of current observations). I assume that the space has 1,000 people and there is 1 person infectious on day 1. The test as a false negative rate of 15%. The prevalence in the outside population is 0.00025 (or 1 in 4,000). I compare testing at the door (no delay) and testing at the desk (1-day delay) with frequencies of 3 and 7 days. The following table gives the number of infections in the population (after 6 months) that arose as a result of internal spread.
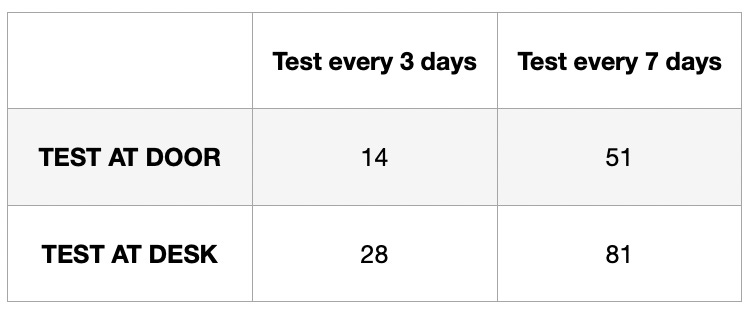
You can see that, for a given frequency, testing at the door results in fewer internally spread infections than testing at the desk. But if testing at the desk can be done more frequently than testing at the door, then you end up with fewer infections. What this means that if testing at the desk is half of the cost, say, of testing at the door, then, for the same cost, you can get fewer infections by testing at the desk.
This is all without doing other things. For instance, contact tracing is someone gets through who is positive or a hybrid system where those who are deemed to be more at risk or work in closed quarters are tested at the door while others are tested at the desk. There are many options available and, for each, we can model the costs and benefits.
The theme here is that we have more options available than a pure focus on minimising the number of infections might yield. When thinking about the whole board of options, a system may involve both lower cost and less risk.