



Welcome to Plugging the Gap (my email newsletter about Covid-19 and its economics). In case you don’t know me, I’m an economist and professor at the University of Toronto. I have written lots of books including, most recently, on Covid-19. You can follow me on Twitter (@joshgans) or subscribe to this email newsletter here. (I am also part of the CDL Rapid Screening Consortium. The views expressed here are my own and should not be taken as representing organisations I work for.)
If someone offered me the AstraZeneca vaccine today, I would take it. I’m 52. That means that in Australia I could be offered AZ but in Canada, I would not be offered it. Isn’t that weird? I feel like I am in a randomised trial of some kind that I did not choose to enter. Interestingly, in Australia, I would be unlikely to find a dose but in Canada, they should be available. Sigh.
How did we end up here? Let’s start with what we seem to know about AZ. In “very rare” instances, AZ has been linked to blood clots. What does that mean?
The safety committee reviewed 62 cases of cerebral venous sinus thrombosis and 24 cases of splanchnic vein thrombosis reported in the European Union’s drug safety databases as of March 22. Eighteen of these cases were fatal. The cases came from the reporting systems of the European Economic Area and the United Kingdom, where 25 million people had received the vaccine.
The EMA estimated that the rare side effect is being reported in 1 in 100,000 people. The UK’s Medicines and Healthcare products Regulatory Agency, or MHRA, gave a slightly lower figure of one case for every 250,000 vaccinations. Both figures could shift as the data, as well as potential causes, are studied.
That’s rare but that presumes we can’t do better in predicting who might be at risk. The earliest study identified the condition in 9 patients, 8 of whom were women with a median age of 36 (range 22 - 49). It also appears that the condition may be treatable but let’s face it, with a mass vaccination roll-out, there is an issue of how people might be identified for treatment. You would need testing for the specific issue which complicates a roll-out considerably.
The straight-out risk equation
This is a nasty issue and it gets nastier when you add some economics. This is from Nature:
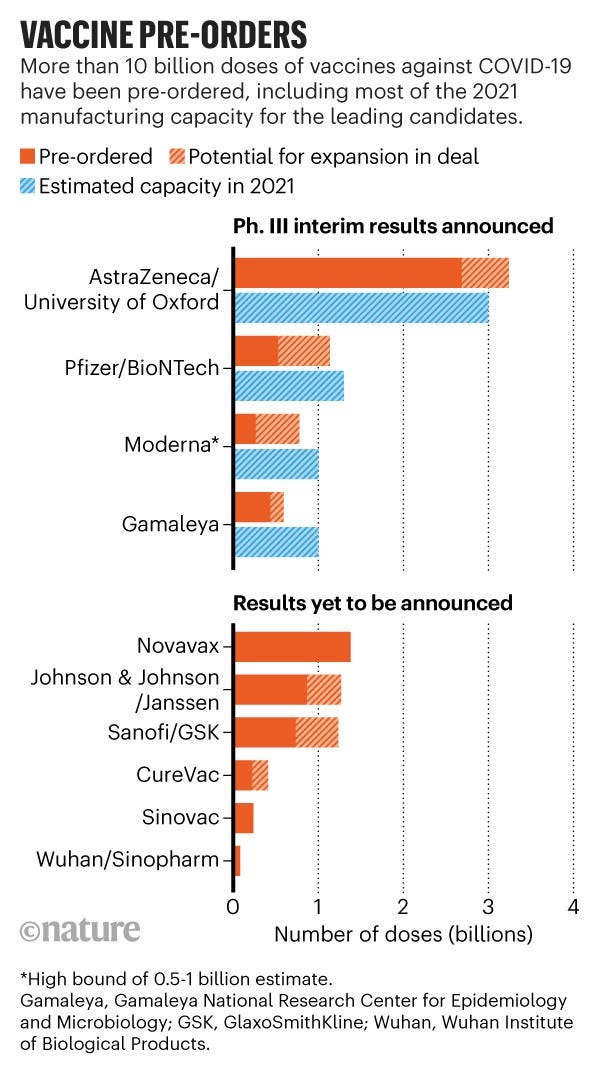
Pre-orders aren’t the same as supply but it is the capacity numbers that are important. World-wide the Covid-19 vaccine means AZ. They will likely cover a third to half of all available doses in 2021 which is when we need them.
So on a straight out distributional basis, the dominant vaccine has a potentially fatal but rare issue. That means that, for most people, not taking AZ means not getting vaccinated in 2021. If you aren’t vaccinated, of course, that means you are at risk of getting Covid-19.
Let’s try, therefore, to assess those risks based on the information we have. First of all, if you are over 50, there does not appear to be anything we could point to as at risk. So we should focus on those under 50. There we have to read the data a little more carefully. Remember 1 in 250,000 people who received AZ in the UK had a blood clotting issue but most of those were over 50. About 20 percent were under 50 (I am using this data but very loosely just to get a sense). Moreover, I am going to guess that half were women. So if you are under 50, your risk of a blood clot problem from AZ was 1 in 50,000 and if you are under 50 and a woman it is more like 1 in 25,000. Of course, it may be that women were disproportionately more likely to receive the vaccine if they were under 50 which means the gender results would have to be more nuanced.
But we have to calibrate this against your Covid risk. Now here things get complicated. But the interesting case is where a country does not give AZ to people under 50 but waits for something else. That will mean 6 months where most of the population are not vaccinated.
This tweet, however, did the comparison.




Only if you are at low risk of exposure, is it even close. Note that as you move from above 50 to below 50 your risk of side-effects moves a whole 1 in one million chance. Based on known data the threshold should be at least under 40 rather than under 55.
On the issue of gender, the evidence is mixed. In the original data, it was disproportionately women who had complications but it may also have been disproportionately women under 50 who received the vaccine. Some additional data suggested that the balance was more like two-thirds women. So AZ should not be given to women under 40 but there is a lower risk for men. Note that, if it turns out that women are at higher risk, not to give AZ to men will put disproportionate costs on women. Not having gender-based policies, in this case, means that you are reducing the available supply of other vaccine candidates to women and allocating them to men who are not at the same level of risk.
We could possibly do even better. Blood clotting in younger people is a Covid-19 effect. What do we know about that? What are the chances that the same people who are susceptible to blood clotting from Covid-19 are the same who have a higher risk from AZ? Is there a way to predict that?
The messaging equation
There is something odd in my mind about the current guidelines on AZ being rolled out. It appears way too conservative with age and needlessly conservative on gender. Given the huge benefits of vaccination along with realistic issues in vaccine supply, the straight-out risk equation doesn’t explain the guidelines to me.
Instead, I suspect this is not about the risk per se but about perceptions and vaccine hesitancy. If people are reluctant to take a vaccine, it is likely because of fear of side effects. Thus, if there are news reports of some people dying (however few) from a vaccine, that isn’t going to help with hesitancy. So I can imagine that public health authorities want to control that news by vaccinating people with no risk.
But that isn’t the margin of the decision here. They are not 100% risk averse otherwise AZ would not be offered at all. Moreover, AZ is very useful for those who are most at risk from Covid-19 fatalities and so there is a balancing act going on. So why choose 55 as a threshold rather than 40? The logic appears to be, maybe the news can be controlled and AZ will still be taken by those most at risk. But there is also another danger that admitting a risk at all is what drives vaccine hesitancy.
In other words, we are in that problematic phase where we are trying to juggle many things. First, balancing real risks is something we can actually measure and do well. Second, balancing the subjective and complicated issue of vaccine hesitancy which is something we know little about let alone how messaging and other factors impact it. What’s worse, vaccine hesitancy is the potentially bigger pandemic management problem.
I think we need to offer a balanced approach. Not have AZ, for the moment, for people under 40. For those between 40 and 55, provide information and allow a choice. And then we have to see how that goes and be ready to adjust based on new information. There is no perfect outcome here. But we need to recognise what we don’t know and push forward — risks in hand.