



Welcome to Plugging the Gap (my email newsletter about Covid-19 and its economics). In case you don’t know me, I’m an economist and professor at the University of Toronto. I have written lots of books including, most recently, on Covid-19. You can follow me on Twitter (@joshgans) or subscribe to this email newsletter here. (I am also part of the CDL Rapid Screening Consortium. The views expressed here are my own and should not be taken as representing organisations I work for.)
When I was writing my first Covid book back in March 2020, my presumption was that if you got Covid or an eventual vaccine, you would be immune and also stop spreading the virus. We didn’t actually know but that was how the experts were talking and, frankly, it was hard to cope with another thought. But I ended up adding a small subsection entitled “What if it’s worse?” to at least cover this possibility.
A report was leaked from the CDC yesterday that I think can be titled “It’s worse.” What has made it worse is Delta. Why?
The viral load measured in vaccinated and unvaccinated people with the Delta variant is almost the same — where it counts in the nose and mouth.
The period of infectiousness is longer (maybe 18 days) than Covid Classic.
The R0 of Delta may be as high as 9.
A silver lining is that vaccination is still preventing serious cases which is very important.
The first part is what worries me. It comes from this slide:
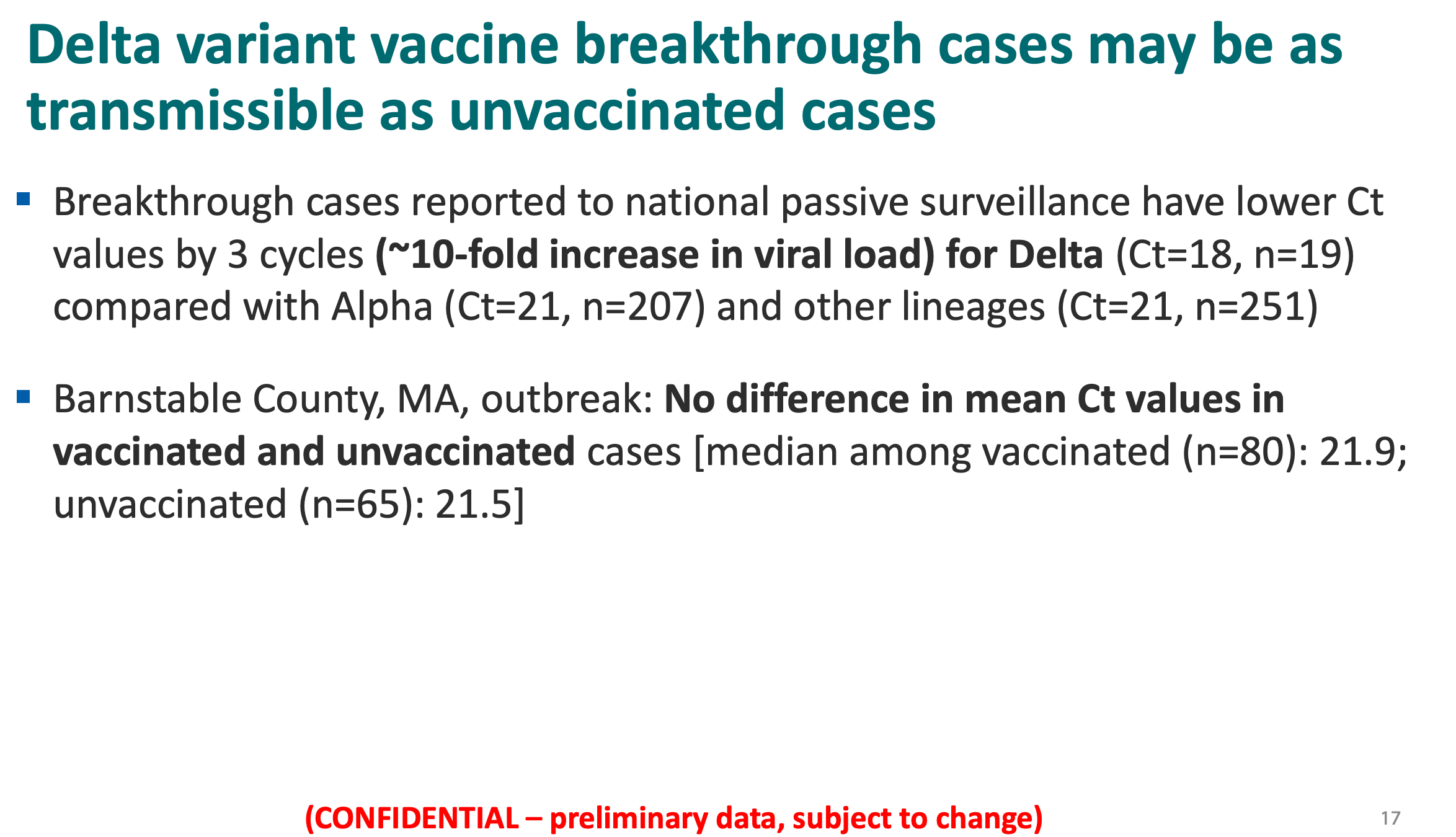
The problem, of course, is this isn’t a lot of data. The sample sizes are really low. There is missing information such as the distribution of viral load (not simply means). And it only deals with mRNA vaccines. This is probably why the CDC didn’t release this report yet. It is worrying but far from conclusive.
This, of course, raises a question — why is the sample size so low? Every case usually has a PCR test and the associated Ct number (which records the viral load — with lower mean orders of magnitude higher viral levels) but the latter isn’t recorded. But if it was collected there would be great information and we could be more confident. But they don’t collect it which continues to suck.
What this means is that we have to take this somewhat surprising result with a grain of salt. But it is appropriate to devote some energy to thinking about what this means if it is true.
First of all, superspreading events where lots of people are indoors at close quarters are still likely to be dangerous. That means that we will need to continue to avoid those circumstances.
Second, moves towards entry credentials that ask for vaccination OR a negative test may well change to just a negative test (or at the very least vaccinated people will have more leeway in terms of the length of time a ‘negative’ test is still valid).
Third, one of the scenarios that motivated us to invest in a rapid screening consortium as an insurance policy for bad pandemic outcomes was that vaccines didn’t stop the spread of the virus. That means that we are going to want to place more weight on rapid antigen screening both in the workplaces, schools and other areas and also for at-home testing. The continued lack of availability of those tests to the general public in Canada is outrageous. In the US, these are sold over-the-counter.
Fourth, the pandemic information problem — that is, identifying infectious people and isolating them — is going to be worse. We have just seen that in Alberta, people who test positive for Covid are no longer required to isolate (although they are advised to do so). Vaccinated people with the sniffles or any other symptoms are, let’s face it, more likely to cast them off as not being Covid when they could very well be that, and of the more transmissible type, too boot. Once again, this raises the need for rapid testing. (And yes I will never let up on this.)
Finally, this is evolutionarily speaking a perfect situation for a virus. You have people who are protected against serious illness but nonetheless can spread the virus. If you were Covid (aka you were playing Covid in the game, Plague Inc), you could not have designed things better to get through to everyone on the planet. But here we potentially are.
We don’t know if it really is worse but the CDC internally seem to think it may be. That will mean that we are not done and that is going to come as a shock. There will be grief about that and, if my Twitter feed, is anything to go by, we are already in the denial phase. Anger will come next and we have already seen how people go on that one during the pandemic.
This newsletter may help you prepare mentally for something I am still hoping we don’t have to prepare for but I don’t really know who I am bargaining with here.